
Albury Wodonga and Region
Advocating for a fit for purpose, future-proofed hospital, to service the people of Albury-Wodonga and surrounds.
Question: Tell me a bit about the advocacy work you were doing for Better Border Health, leading up to the election on the weekend.
Answer:
Better Border Health’s focus leading into the Farrer by-election was very clear: we wanted voters to understand where each candidate stood on the future of Albury Wodonga Health and, in particular, whether they supported a genuinely fit-for-purpose new public hospital on a new single site.
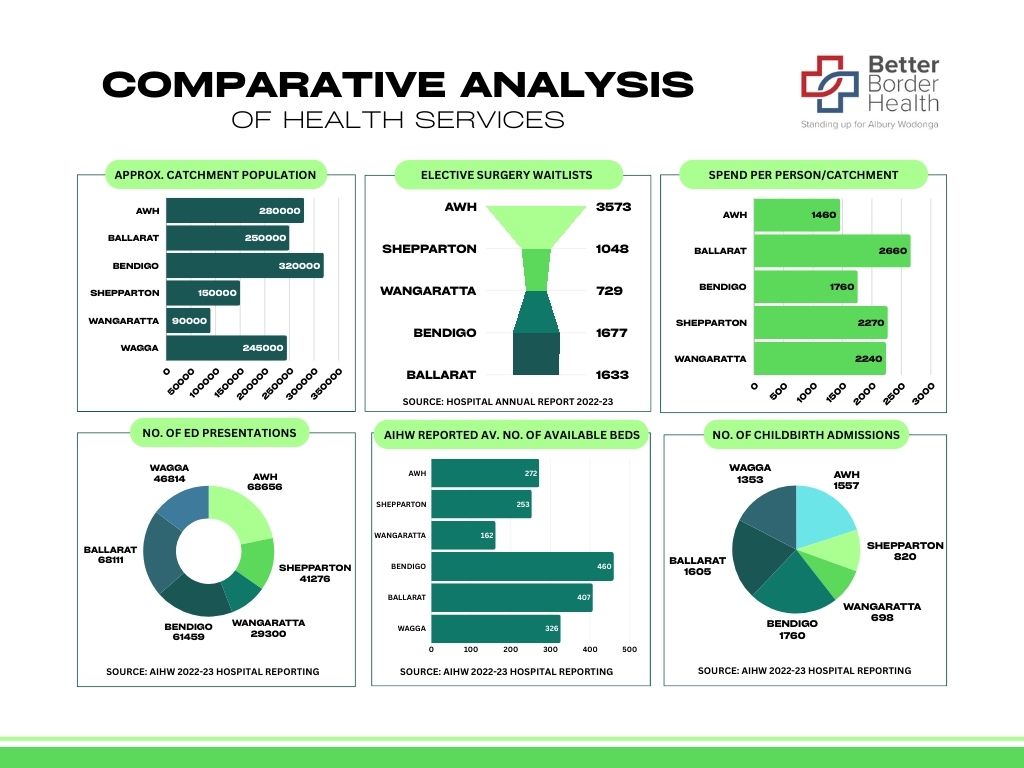
This is not a minor local issue. Albury Wodonga Health serves a catchment of around 300,000 people across the NSW–Victoria border and provides care to communities representing roughly half of the Farrer electorate. It is the clinical lifeline for a huge inland region, yet it is still being asked to function with infrastructure, funding and bed capacity that fall well short of what comparable regional centres receive.
We highlighted the positions of all candidates, especially in relation to whether they backed the community’s call for a new hospital on a new site or whether they supported continuing with the current brownfield redevelopment on the Albury campus. That redevelopment does not go close to meeting our community’s current needs, let alone its future needs.
We did receive a lot of criticism, particularly from One Nation supporters, after we urged voters who support a new public hospital on a new site to place David Farley last on their ballot paper. But our position was based on the hospital issue, not party politics. Mr Farley supported the existing redevelopment path, serious questions remained about comments he had made regarding private involvement in the hospital system, and he had not met with local clinicians. We believed voters deserved to know that.
We also understand why there was a protest vote. Rural and regional communities have been neglected for decades, and people are angry. The political system has been resoundingly rejected by many voters. But our concern is that this protest vote has delivered an outcome that may not advance the urgent hospital solution our community needs.
Question: Did candidates prioritise healthcare infrastructure enough during the campaign process?
Answer:
Most candidates did acknowledge that Albury Wodonga Health is in crisis and that healthcare infrastructure was a central issue in this campaign. There was broad recognition from many candidates that the current proposal is inadequate and that the region deserves more than a compromised redevelopment.
Independent candidate Michelle Milthorpe and Greens candidate Richard Hendrie supported halting the current proposal and returning to the greenfield hospital model recommended in the 2021 Clinical Services Plan and Masterplan. That position aligned with the advocacy of local clinicians and the broader community campaign.
The Coalition also acknowledged gaps in the current redevelopment and made further commitments toward addressing those gaps, including planning for a future greenfield hospital.
The exception was One Nation candidate, David Farley. In our view, he did not prioritise healthcare infrastructure in the way this crisis demands. He supported continuing with the brownfield redevelopment despite strong community and clinician opposition, and despite Justice Richard Beasley’s findings that the current project is unlikely to meaningfully address bed shortages. He also made comments around private involvement in the hospital system that raised serious concerns, and he had not engaged with local clinicians in the way we would expect of someone seeking to represent a region in the middle of a healthcare crisis.
That is why Better Border Health advocated for him to be placed last by voters who support a new public hospital on a new site.
Question: Are you happy with the election outcome? Why or why not?
Answer:
No, we are not happy with the outcome from a health advocacy perspective.
We understand the anger that drove the protest vote. People in regional communities are tired of being ignored, and many voters clearly wanted to send a message to the major parties. We do not dismiss that frustration at all. In fact, much of our campaign has been about calling out exactly that neglect.
But based on David Farley’s position on Albury Wodonga Health, we do not believe this is a good outcome for our hospital campaign. He has shown scant regard for the community’s call for a new public hospital on a new site. He supported the existing brownfield redevelopment, despite the 2021 Clinical Services Plan recommending a greenfield option and despite the findings of Justice Beasley’s inquiry raising serious concerns about the adequacy of the current plan.
We are also concerned about his comments around privatisation or private involvement in the hospital system. Albury Wodonga Health must remain a strong, properly funded public health service. Our community should not be forced into private-sector solutions because governments have failed to fund and plan properly.
We are also deeply concerned about the broader impact of One Nation’s rhetoric around migration. Rural health services are heavily reliant on migrant doctors, nurses and specialists. In rural Australia, 41 per cent of doctors are migrants, and one in 16 doctors are from Islamic countries. Locally, in places such as Corowa and Howlong, 83 per cent of doctors are migrants and 33 per cent are from Islamic countries.
These doctors are not peripheral to rural healthcare; in many communities, they are literally holding the system together. Several local doctors have already contacted us to express concern about One Nation’s win in Farrer, and some are considering leaving. That is a serious workforce risk for a region already struggling to recruit and retain clinicians.
So while we understand why people voted the way they did, we are very concerned about what this result means for the future of Albury Wodonga Health and for the health workforce our community depends on.
Question: Do you have confidence that David Farley will prioritise Albury’s lacking infrastructure?
Answer:
Based on the evidence to date, no, we do not.
Albury Wodonga Health is one of the most urgent infrastructure failures in regional Australia. It serves a catchment of around 300,000 people, sits around four hours from the nearest tertiary referral hospital, and provides care to communities representing about half of the Farrer electorate. Any local member representing this region should be fighting relentlessly for a fit-for-purpose public hospital.
Mr Farley has not demonstrated that commitment. He backed the existing brownfield redevelopment, even though local clinicians, community advocates and councils have been clear that it is not enough. He has not supported the community’s call for a new public hospital on a new site. He has also made comments around private involvement that create real concern about the future direction he would support.
The current redevelopment has already been heavily criticised. Justice Richard Beasley’s report into NSW healthcare funding found that the funding approach for Albury Wodonga Health was not properly based on the 2021 Clinical Services Plan or a thorough assessment of clinical need. The report also warned against designing major health infrastructure around a predetermined funding amount rather than around what patients and clinicians actually require.
That is exactly what our community fears has happened here. We have a project being presented as a solution, when the evidence says it will not solve the core problems.
So no, at this point we do not have confidence that David Farley will prioritise Albury’s infrastructure crisis in the way the community needs.
Question: How do you plan to keep the pressure on the government and local MP now that the election spotlight might start to fade?
Answer:
We will do what we have always done: keep telling the truth about how badly this community has been short-changed.
The Farrer by-election gave Albury Wodonga Health national attention, but the crisis does not disappear because the campaign is over. Patients are still waiting. Ambulances are still ramping. Staff are still working in overstretched conditions. Beds are still unavailable. People are still being forced to travel for care that should be available in a regional centre of this size.
We will continue to compare Albury-Wodonga with the regional health services it should be benchmarked against. Bendigo and Ballarat are our main comparators. They are the most relevant peer services in terms of scale, catchment and role. Yet Albury-Wodonga is nowhere near on equal footing with them when it comes to recurrent operational funding.
Based on the 2024/25 annual reports, Albury Wodonga Health received $173 million less funding than Bendigo and $255 million less funding than Ballarat in the last financial year. That is the operational inequity in plain terms. Albury-Wodonga is being asked to carry the workload of a major inland regional health service while being funded materially below its closest peers.
AWH was described at its AGM as the second-busiest regional health service administered by Victoria, behind only Geelong. That makes the funding gap with Bendigo and Ballarat even harder to justify.
We will also keep highlighting the practical consequences of underfunding and inadequate infrastructure. Albury-Wodonga is the largest regional community in Australia without 24/7 heart attack coverage. It is the largest regional community in Australia without a helipad. It has only nine dialysis chairs, compared with 24 in the much smaller Wagga Wagga, and more than 20 in both Bendigo and Ballarat. That is why Dr Russel Auwardt has warned that some people are effectively choosing to die rather than continue with the burden of accessing dialysis.
We will continue to speak publicly, support clinicians, brief media, engage with governments, and call out any attempt to pretend this redevelopment is enough. Albury-Wodonga is not asking for special treatment. It is asking to be funded and planned for on something approaching the same footing as its main comparator services.
Question: For those unfamiliar with Albury’s infrastructure issues, can you please explain the situation and how dire it is?
Answer:
Albury Wodonga Health is not just another regional hospital. It is the major health service for a cross-border catchment of around 300,000 people and is approximately four hours from the nearest tertiary referral hospital. It serves communities across both Victoria and NSW and provides care to around half of the Farrer electorate.
The service is now under extreme pressure. Daily bed shortages, ambulance ramping, makeshift clinical spaces, and long elective surgery waiting lists have become routine. GPs are telling us they are seeing patients every day who cannot access the hospital care they need. Patients and families are increasingly worried that delays in care are contributing to avoidable harm.
The core issue is that the region has outgrown the infrastructure and funding it has been given.
The 2021 Clinical Services Plan and Masterplan provided a clear pathway forward. It recommended a new greenfield hospital because that option offered the best chance of delivering the capacity the region needs, while also reducing the risks of trying to build around active hospital services.
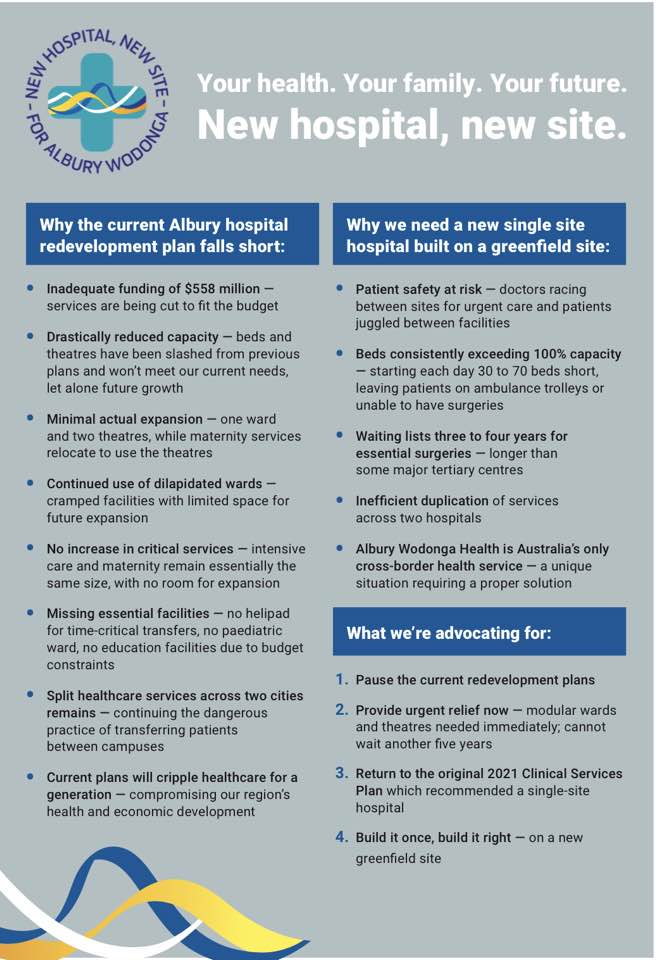
In 2022, the Victorian and NSW governments announced $558 million for Albury Wodonga Health. That announcement was presented as a major step toward a single-site, centre-of-excellence hospital on the Albury campus. But since that announcement, the promised outcome has been repeatedly reduced in scope. What is now being pursued is a compromised brownfield redevelopment that falls far short of what was promised and what the region needs.
More than 200 local doctors wrote to all levels of government in October 2024, including the Prime Minister, warning that the redevelopment was inadequate and calling for urgent intervention. Their concerns have since been supported by major professional bodies, including the Australian Medical Association, the Rural Doctors Association of Australia, and the NSW Nurses and Midwives’ Association.
Justice Richard Beasley’s 2025 report from the NSW Special Commission of Inquiry into Healthcare Funding added further weight to those concerns. The report criticised the way the redevelopment funding was developed, including concerns that it was not properly based on the 2021 Clinical Services Plan or a thorough assessment of need. It also warned against designing major health infrastructure around a fixed funding amount rather than clinical requirements, because that risks both patient safety and public money.
The bed numbers show how serious the problem is. According to the Australian Institute of Health and Welfare, Albury Wodonga Health has 272 acute inpatient beds. Bendigo has 460 and Ballarat has 407. Those are our main comparator services, yet Albury-Wodonga is operating with far fewer acute inpatient beds.
The current redevelopment is often promoted as delivering 110 additional overnight beds, but that headline figure includes emergency department and mental health beds. Those beds are important, but they do not solve the acute inpatient bed shortage — the medical and surgical overnight beds that allow patients to move safely out of the emergency department and into wards.
Analysis by the Border Medical Association and Better Border Health indicates that, once emergency beds and mental health beds are excluded, and once the reduction in acute inpatient beds at Wodonga is accounted for as acute services are consolidated onto the Albury campus, the net increase in acute inpatient beds is only around 35. That is below the current shortfall and nowhere near future need.
AWH is currently operating at around 110 to 125 per cent occupancy and is short 40 to 70 beds daily. That is well beyond accepted safe hospital flow levels. The Australasian College for Emergency Medicine has argued that access block would largely cease to be a problem if bed occupancy were reduced to about 85 per cent, and the Medical Journal of Australia has also identified occupancy above 85 per cent as undermining safe and efficient hospital operation.
On that benchmark, Albury-Wodonga is not simply busy. It is operating in sustained overload.
The situation is dire because this is not an isolated inconvenience. It affects whether a patient can get a bed after presenting to emergency. It affects whether ambulances can unload patients and get back on the road. It affects whether elective surgery goes ahead. It affects whether specialists stay. It affects whether GPs are left managing patients in the community who should be in hospital. And it affects whether families can trust that care will be available when they need it.
That is why the community is fighting so hard. We are not asking for luxury. We are asking for a safe, properly funded, future-proofed public hospital for one of the largest inland regional communities in Australia.
Rally for our hospital!
11am, Monday 27 April – QEII Square, Albury
See speaker Stan Stavros, director Better Border Health
Farrer byelection Q&A: where do the candidates stand on health – The Border Mail – 24 April 2026

Do you want to revisit the Better Border Health candidates’ forum on 22 April 2026?
Here is the link to the recording.
Stop the Spin! Publish the real number of extra acute beds
13 April 2026
Albury Wodonga Health (AWH) and Health Infrastructure NSW (HI) continue to promote an “uplift of 110 beds” as part of the hospital redevelopment.
In July 2025, AWH Chair Jonathon Green and CEO Bill Appleby issued a “Setting the Record Straight” media release stating that “the current project scope is forecast to deliver an uplift of 110 beds”.
To most people, that sounds like relief is on the way. But our community is sick of headlines and half-truths.
We want one plain answer:
How many extra acute inpatient beds will we actually get, net, once all closures and removals are counted?
Why acute inpatient beds matter
An acute inpatient bed is a hospital bed for someone who is seriously unwell or injured and needs to be admitted for urgent treatment and close monitoring, often coming from the Emergency Department. These are the beds used for strokes, heart attacks, pneumonia, serious infections, major injuries, and care after surgery.
When acute inpatient beds are short, everything jams up:
- ED fills and people wait far too long
- Ambulances can’t offload
- Planned surgery is delayed
- Staff are forced to use “overflow” areas not designed for patient care
The reality right now
AWH is operating at 110 to 125 per cent capacity, even though safe-care guidelines recommend no more than 85 per cent.
Daily bed deficits are now frequently between 40 and 70, based only on expected intake, and not counting those who give up, travel elsewhere, or have surgery delayed.
And the deficit isn’t standing still. It is growing year on year because we live in one of the fastest-growing regions in Australia.
What Justice Beasley said: spend based on need, or it’s wasted
The NSW Special Commission of Inquiry into Healthcare Funding, led by Justice Richard Beasley, warned that health infrastructure spending must be based on what the community needs, not “the money said to be available”.
He also found there was little evidence the proposed Albury Hospital redevelopment was based on the kind of proper analysis needed to match a growing catchment’s health needs.
In plain English: if you spend hundreds of millions without properly planning for current and future demand, that is how you end up wasting money.
How “110 beds” becomes a much smaller number of extra acute beds
This is the part our community deserves explained clearly.
The “110 beds” headline includes beds that are not acute inpatient ward beds, and it ignores beds that will be lost when services shift and temporary overflow areas are shut down.
So, to estimate the real net gain in acute inpatient beds, we do a simple what’s added minus what’s taken away.
Start with the headline
- 110 beds (promoted uplift)
Subtract beds that are not extra acute inpatient ward beds
- Minus 14 Emergency Department beds (ED beds are not inpatient ward beds)
- Minus 8 mental health beds increase (important, but not extra acute medical/surgical beds)
- Minus 2 dialysis chairs replacing 2 beds in Ward 2 (a swap, chairs replacing beds is not a bed increase)
Subtract beds that won’t be available to acute inpatients
- Minus 9 cancer centre beds currently used by AWH.
AWH has confirmed these beds will return to support the growing number of patients requiring cancer services. Dr Brett Hamilton, Clinical Director of Cancer Services, AWH, has confirmed that conjecture about retaining these beds is unfounded.
- Minus a further 10 temporary overflow beds currently commissioned in areas such as former tea rooms and transit lounges, to be decommissioned when the new tower opens.
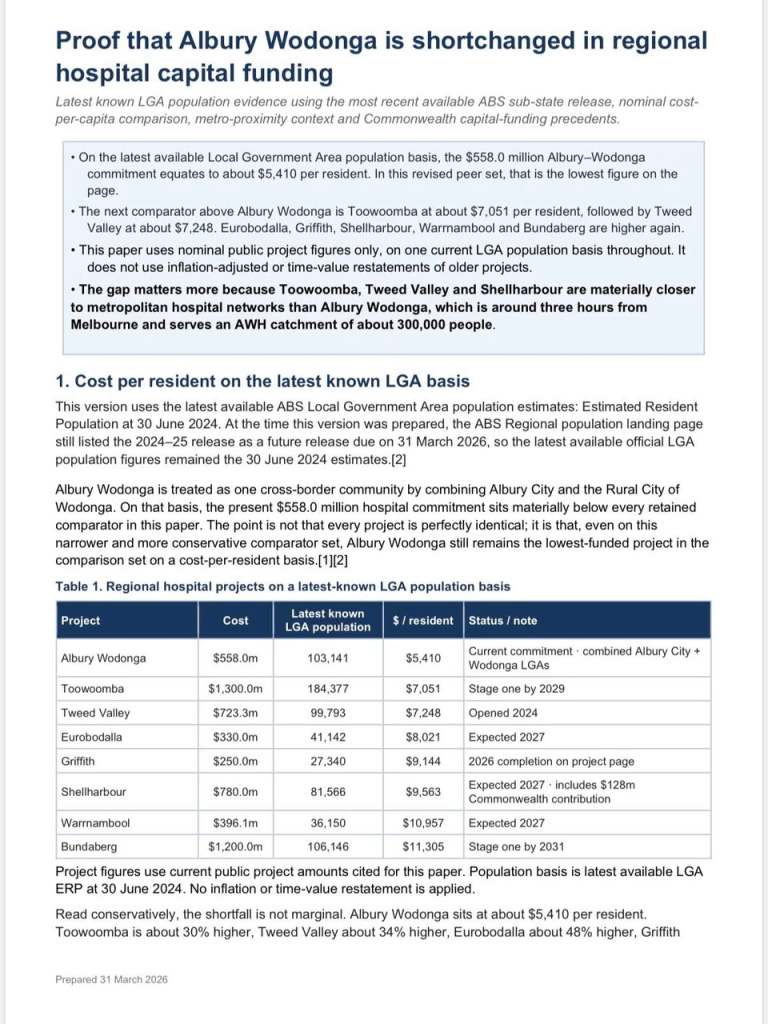
Proof that Albury Wodonga is shortchanged in regional hospital capital funding
1 April 2026
A new analysis (see following) by Better Border Health highlights a significant inequity in regional hospital capital investment affecting Albury Wodonga
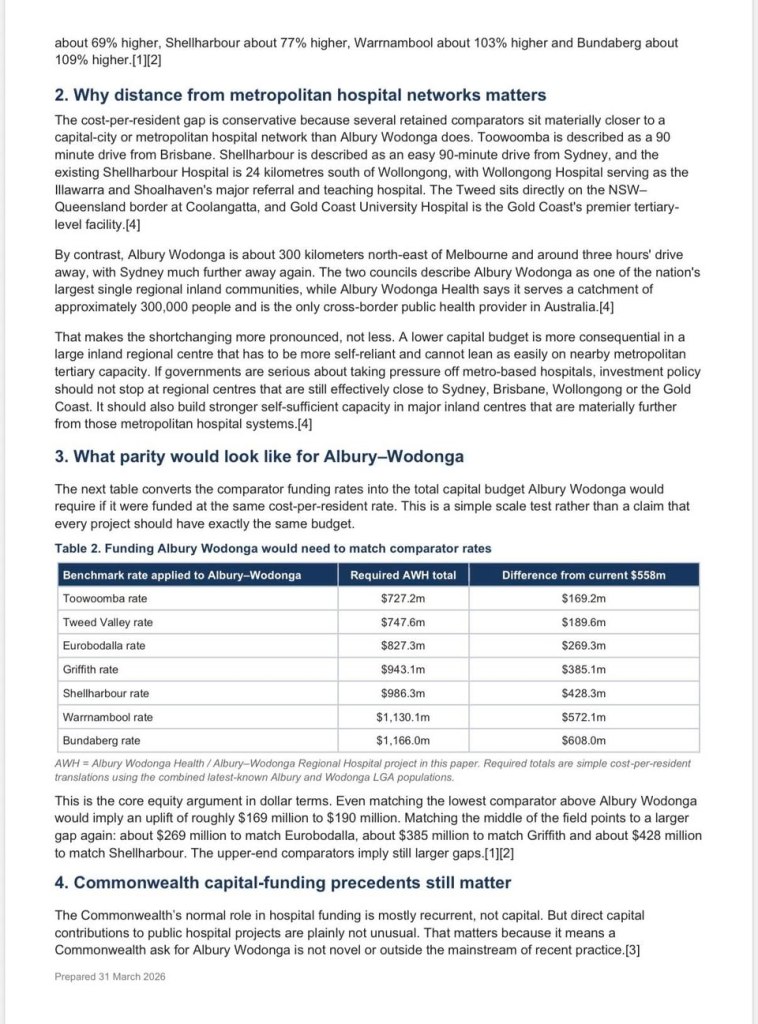
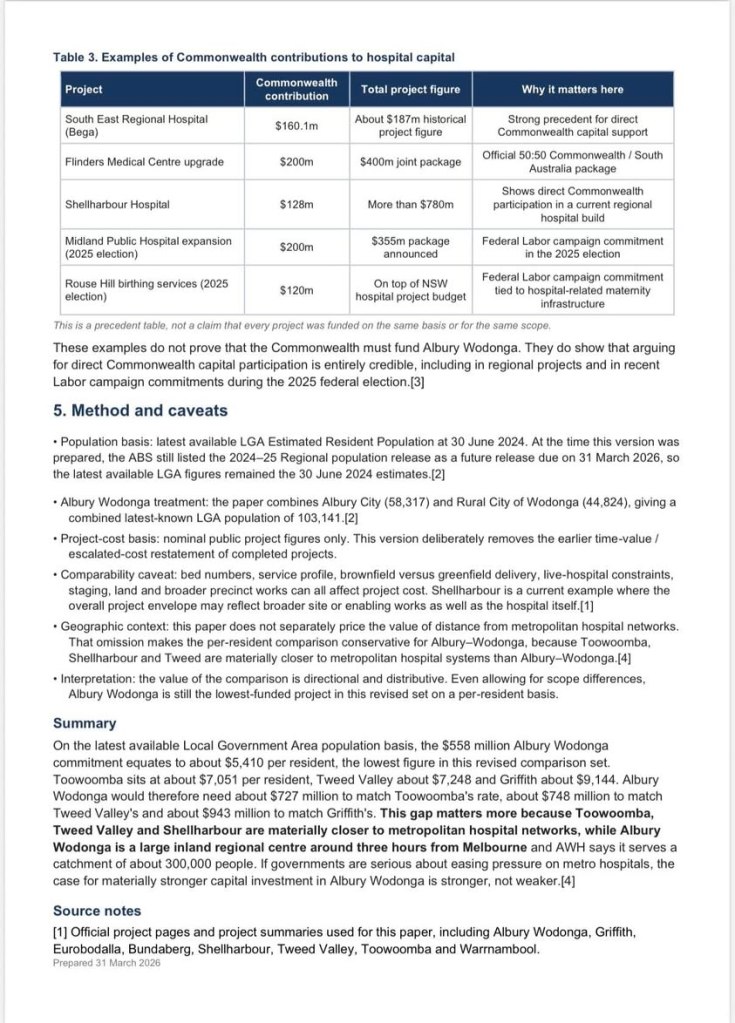
Using the latest available Local Government Area population basis, our analysis shows that Albury–Wodonga’s combined hospital commitment of $558 million equates to approximately $5,410 per resident. This sits materially below a number of comparator regional hospital projects, including Toowoomba ($7,051 per resident), Tweed Valley ($7,248), Eurobodalla ($8,021), Griffith ($9,144), Shellharbour ($9,563), Warrnambool ($10,957) and Bundaberg ($11,305).
In Better Border Health’s view, this gap is even more concerning when considered in context. Several comparator centres, including Toowoomba, Tweed Valley and Shellharbour, are substantially closer to major metropolitan and tertiary hospital networks than Albury Wodonga. By contrast, Albury Wodonga is a major inland regional community that must be significantly more self-reliant while also serving a large cross-border and regional population.
This analysis therefore reinforces what our community experiences on a daily basis: the inequity is not limited to capital funding alone. It is also reflected in the broader pressures facing our health service, including recurrent funding constraints, bed shortages, the absence of 24/7 heart attack coverage, limited operating theatre capacity and insufficient dialysis chairs when compared with other regional centres.
Taken together, these issues point to a health system that is being asked to do more with less.
If governments are serious about improving regional healthcare and easing pressure on metropolitan hospitals, then investment decisions must better reflect the realities faced by large self-reliant regional centres such as Albury Wodonga.
This issue now requires strong and united advocacy. All local politicians, state and federal, on both sides of the border, should stand up for Albury Wodonga and secure the level of hospital investment this region needs and deserves.
Alliance of Councils Advocacy Document – April 2025
Proof our Border community is missing out
15 November 2024
Support us
Scan the QR code OR click the links below:

